Key takeaways:
- It took as much as 16 years to de-implement pointless cervical most cancers screenings.
- Many males are nonetheless unnecessarily screened for prostate most cancers regardless of a change in steering in 2012.
Stopping pointless most cancers screenings can take over a decade after new pointers are launched, based on a overview revealed in BMJ High quality & Security.
“Extreme screening opens the door for a whole lot of adverse penalties,” Jennifer H. LeLaurin, PhD, an assistant professor of well being outcomes and biomedical informatics on the College of Florida, stated in a press launch. “These pointers are based mostly on what the advantages and harms are. If the harms outweigh the advantages for a selected take a look at, then they suggest towards it.”

LeLaurin and colleagues assessed six U.S. Preventive Providers Job Power most cancers screening suggestions and measured the time between guideline publication and de-implementation, outlined as a 50% discount in the usage of the observe in routine care.
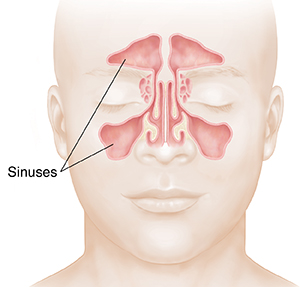
They discovered that the time it took to de-implement cervical most cancers screening was 4 years for girls aged youthful than 21 yearsand 16 years for girls aged older than 65 years.
In the meantime, prostate screening in males aged 70 years or older has not but reached the de-implementation mark because the process pressure’s 2012 guideline launch.
Healio spoke with LeLaurin to study extra concerning the findings, how physicians can navigate ambiguous screening conditions, and extra.
Healio: Did any findings notably stand out to you? What ought to well being care suppliers in the end take away from the info?
LeLaurin: One of many shocking findings was the variability within the tempo of de-implementation. For instance, nonrecommended cervical most cancers screening beneath age 21 years was pretty speedy, whereas prostate most cancers screening in older males continues to be quite common. For HCPs, I feel the takeaway is that holding updated on observe pointers is important, however on a bigger scale we want different methods to successfully change observe. This may embody media campaigns, high quality measures, modifications to reimbursement insurance policies and different multilevel methods.
Healio: If the USPSTF now not recommends a sure screening, what are the implications for insurance coverage cowlage? Would it deter suppliers from referring sufferers to these screenings?
LeLaurin: Whereas USPSTF Grade D suggestions can affect insurance coverage protection, it isn’t at all times persistently aligned. For instance, Medicare covers prostate most cancers screening for males over 50, with out an higher age restrict. So, whereas lack of protection could deter some referrals, it’s usually not ample to cease low-value practices by itself.
Healio: What ought to physicians do in conditions the place a affected person does not meet screening necessities however nonetheless needs to endure screening?
LeLaurin: This is a vital alternative for shared decision-making. Whereas evidence-based pointers advise towards screening in sure age teams, selections about screening ought to nonetheless be individualized based mostly on affected person values, considerations and well being historical past. Physicians ought to take heed to sufferers’ considerations but in addition educate them on the steadiness of advantages and harms, like false positives and pointless invasive procedures. Emphasizing that not screening is supported by robust proof may help reframe the choice to not display screen as evidence-based observe slightly than denial of care. Instruments like choice aids could assist navigate these conversations.
Healio: The place does analysis on pointless most cancers screenings, and methods for lowering these, go from right here?
LeLaurin: We want higher infrastructure for measuring and monitoring low-value care over time. Present knowledge techniques are likely to concentrate on underuse of beneficial providers slightly than overuse of low-value ones. Increasing nationwide surveillance and integrating extra low-value care measures into high quality metrics may assist. Additionally, extra implementation analysis is required to grasp which methods, akin to scientific choice help instruments and efficiency monitoring, are only in selling de-implementation of particular practices.
Healio: The rest you’d wish to add?
LeLaurin: It’s essential to emphasise that the USPSTF pointers we examined on this research solely apply to sufferers who’re asymptomatic. If a affected person presents with signs in step with prostate, cervical or different cancers, physicians ought to observe applicable diagnostic procedures. Our work additionally underscores that de-implementation shouldn’t be merely the other of implementation. It requires its personal set of methods, knowledgeable by proof, context and stakeholder engagement.
References:
For extra info:
Jennifer H. LeLaurin, PhD, may be reached at primarycare@healio.com.