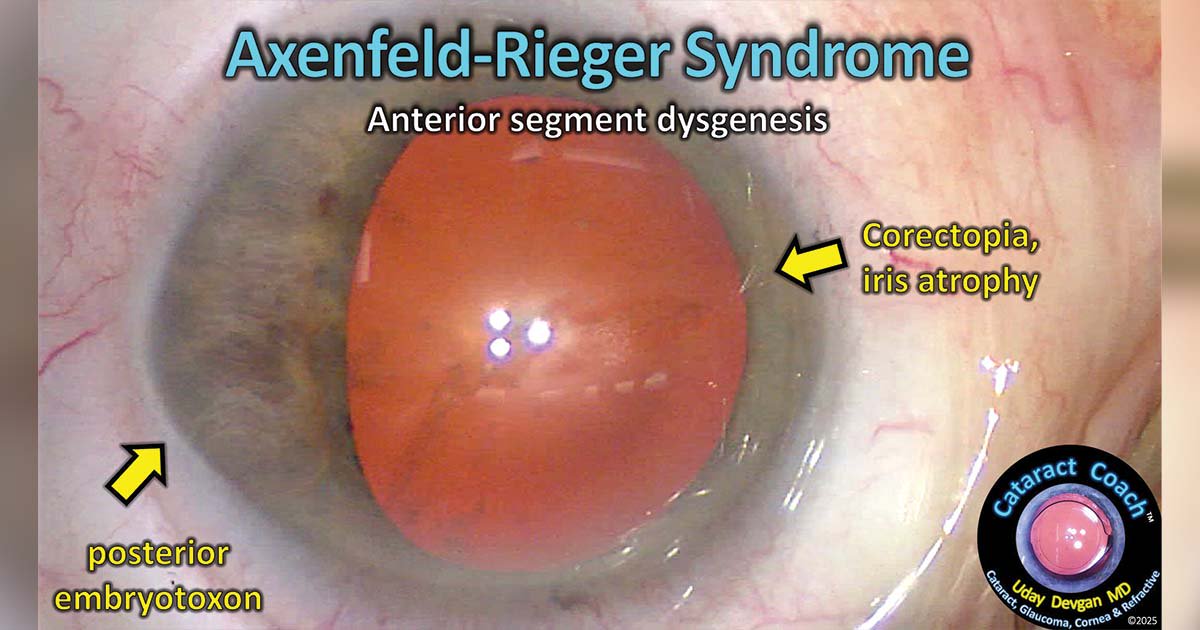
A century in the past, Theodor Axenfeld described a sequence of sufferers with congenital abnormalities of the anterior phase of the attention, together with anterior displacement of Schwalbe’s line, termed posterior embryotoxon, with anterior iris adhesions.
Shortly thereafter, Herwigh Rieger famous extra iris abnormalities equivalent to corectopia, polycoria and iris atrophy in these sufferers together with systemic deformities of tooth and facial bones.

Supply: Uday Devgan, MD
As a result of dysgenesis of the anterior phase, the attention is susceptible to extra pathology equivalent to growth of glaucoma resulting from irregular angle anatomy. Luckily, Axenfeld-Rieger syndrome is uncommon, and the diploma of structural abnormalities can differ alongside a spectrum from delicate to extreme.
A affected person was referred to our clinic for cataract surgical procedure, and a substantial period of time was spent evaluating the attention, with care taken to detect the presence of confounding elements that would complicate the process. The affected person was famous to have an uncommon corneal form that appeared considerably rhomboid (Determine 1). The posterior embryotoxon was seen in sure areas of the cornea, and notably there was corectopia with decentration of the pupil upon dilation resulting from an space of iris atrophy. No glaucoma was current, and the angle anatomy appeared affordable with only some areas famous to have iris strands adherent to Schwalbe’s line.

Uday Devgan, MD
In instances of Axenfeld-Rieger syndrome, it is not uncommon to have zonular laxity with focal areas of zonular absence, significantly within the space of iris atrophy. Whereas our affected person appeared to have a standard diploma of zonular help, that is higher assessed throughout surgical procedure. Because of this, we organized to have further instrumentation out there within the working room, equivalent to capsule hooks, a capsular stress ring, a capsular stress phase and the suitable sutures. This affected person was additionally extremely myopic with an extended axial size and desired to take care of a average diploma of myopia to permit for unaided close to imaginative and prescient. IOL calculations have been carried out for the affected person’s most popular refractive goal, and a toric monofocal IOL was chosen as the primary selection. We additionally organized to have a three-piece monofocal IOL, which solely is available in non-toric variations, out there as a back-up plan.

Supply: Uday Devgan, MD
Within the working room, we began with topical tetracaine and intracameral preservative-free lidocaine for anesthesia, together with some delicate systemic sedation with midazolam. If the case turned extra sophisticated, we may all the time complement that with a sub-Tenon’s administration of further native anesthetics to realize analgesia and akinesia. The incision was made temporally as a result of that was the world of the cornea that was farthest from the visible axis. A superior incision on this case can be nearer to the visible axis, and that may seemingly induce extra astigmatic impact.
The preliminary creation of the capsulorrhexis provides vital clues as to zonular laxity if we begin it by puncturing the lens capsule with our forceps. If we use a pointy needle or cystotome as an alternative, there’s little suggestions as to how taut the anterior capsule is. Luckily, the zonular help appeared regular, and we may proceed with the capsulorrhexis. Importantly, the capsulorrhexis was centered on the capsule and never throughout the pupil. Due to the uneven pupil dilation, we wished to keep away from utilizing the pupil margin as a information for the capsulorrhexis as a result of it might lead to a misaligned anterior lens opening. (Determine 2)

Supply: Uday Devgan, MD
The nucleus removing went easily on this case, utilizing a phaco chop variation. Throughout cortical cleanup, care was taken to watch the capsulorrhexis to make sure that it didn’t transfer. For a full 360°, the zonular help was sturdy, so a capsular stress ring was not wanted. We implanted a toric monofocal IOL that was aligned on the applicable axis to handle the corneal astigmatism. Due to the care taken to create the capsulorrhexis, there was an entire 360° overlap of the IOL optic, which was effectively centered within the affected person’s visible axis (Determine 3).
The affected person achieved a wonderful postoperative final result and healed effectively from the surgical procedure. She is being referred again to retina and glaucoma colleagues who will observe her longitudinally. For this affected person, happily the diploma of ocular abnormalities from Axenfeld-Rieger syndrome was restricted, and the cataract surgical procedure was uneventful for each eyes. As a result of it is a uncommon situation, occurring in lower than one in 100,000 folks, I’ll not see one other affected person with this situation within the second half of my profession.
A video of this may be discovered at https://cataractcoach.com/class/unusual-cases/.
For extra data:
Uday Devgan, MD, in non-public apply at Devgan Eye Surgical procedure and a companion at Specialty Surgical Heart in Beverly Hills, California, could be reached at devgan@gmail.com; web site: www.CataractCoach.com.
Sources/Disclosures
Collapse
Professional Submission
Disclosures:
Devgan reviews proudly owning and working CataractCoach.com, which is a free useful resource for ophthalmologists, and being a principal in RetinaRounds.com, which can also be a free useful resource.